
$50 Billion for Rural Health: Where to Put It to Work
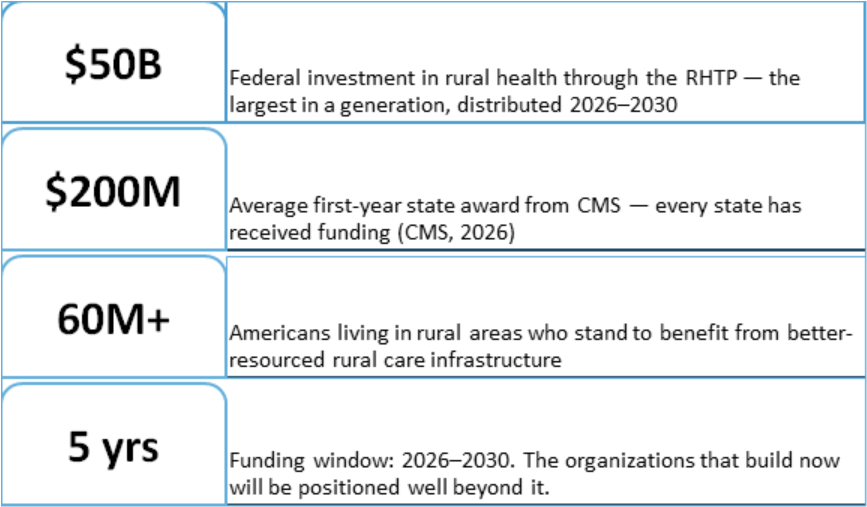
The Rural Health Transformation Program (RHTP) is $50 billion in federal investment directed at exactly the communities that need it most. For rural hospital leaders and health system executives who move quickly and invest strategically, it is the most significant opportunity to reshape rural care delivery in a generation.
Established under the One Big Beautiful Bill Act and administered by CMS, the RHTP distributes $10 billion per year from fiscal year 2026 through 2030. Every state has received a first-year award averaging $200 million. The fund is purpose-built for transformation: telehealth expansion, workforce development, technology modernization, chronic disease programs, and innovations in care delivery that improve access and outcomes for rural residents. States can also direct up to 15% of their award toward direct provider payments — targeted support for facilities providing services in areas with the greatest access gaps.
The rural health leaders best positioned to use this funding are the ones who treat it as a strategic planning catalyst — not a stopgap — and who align their investments with the care model their communities will need for the decade ahead. That requires clarity about where the highest-impact opportunities are and how RHTP funding can be structured to support them.
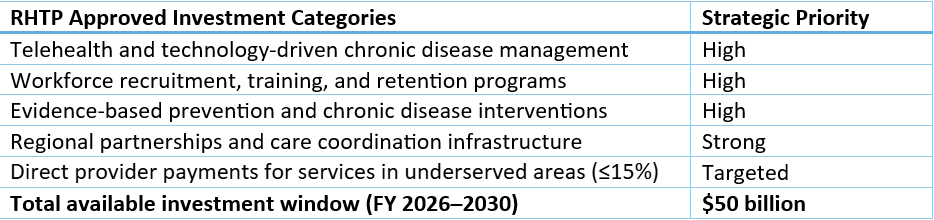
The RHTP funds are organized around five approved investment categories, each of which maps directly to the structural gaps that have made rural health delivery challenging for decades. Half of funding is distributed equally among all approved states; the other half is allocated by CMS based on rural population, facility proportion, and need. States can also direct up to 15% of their award toward direct provider payments for services in underserved areas — a meaningful targeted tool for facilities with the highest community dependence. The fund is designed to reward states and health systems that bring a coherent transformation strategy, not incremental requests. That is exactly the kind of strategy that rural health leaders should be building now.
States are required to submit transformation plans outlining how they will use their awards across these categories. The plans that are succeeding — and attracting the highest CMS support — are those that tie investments directly to measurable access and outcomes improvements. For rural health systems and critical access hospitals, this means the most competitive position is one where you have already done the internal analysis: which service lines need investment to reach their potential, where your workforce gaps create the greatest access risk, and what technology infrastructure would most meaningfully expand the care you can deliver to your community.
The RHTP is designed to fund solutions, and the highest-impact investment opportunities map directly to the service areas where rural communities have the greatest unmet need. For rural hospital leaders developing their state's transformation plan or positioning their organization to receive a share of state awards, these are the categories where investment produces the clearest access and financial returns.


State transformation plans vary significantly in how they prioritize RHTP investments — and individual rural hospitals have a meaningful opportunity to shape those priorities at the state level. Engaging early with your state health department and Medicaid office on how RHTP funds will be allocated is not a bureaucratic exercise. It is one of the most consequential strategic conversations your leadership team can have in the next 12 months.
Accessing RHTP funds is the first step. Building care model improvements that generate sustainable value beyond the funding window is the objective. For rural health leaders, that means pairing the investment with operational architecture — the design, workflow, and partnership structures that allow transformation investments to produce lasting results rather than one-time infrastructure upgrades.
Start with a service line investment map, not a budget request. The RHTP rewards transformation strategies that are specific, measurable, and tied to community access outcomes. Before pursuing state award funds, rural health leaders should conduct a rigorous, data-driven assessment of their service line portfolio: which services have the highest community dependence and the most viable financial model with investment, which could be restructured through telehealth or regional partnership to become sustainable, and which require a new delivery model entirely. Organizations that arrive at state planning conversations with that analysis in hand are far better positioned to receive and deploy funds effectively.
Invest in workforce retention as aggressively as recruitment. RHTP workforce funds are most commonly discussed in the context of recruitment — loan repayment, residency programs, and pipeline development. These are valuable. But the highest near-term return on workforce investment is retention. At $61,000 per RN replacement and $295,000 per 1% shift in turnover rate, reducing attrition by even a few percentage points produces savings that more than offset the cost of retention programs. Scheduling redesign, care team models that reduce administrative burden, leadership development for front-line managers, and competitive compensation benchmarking are all investable with transformation funds — and all produce returns that compound across the five-year window and beyond.
Use the RHTP to formalize regional partnerships before the market does it for you. The RHTP explicitly funds regional health partnerships — and this is one of its most strategically valuable, approved uses. Rural hospitals that proactively build co-management agreements, shared specialty service arrangements, and telehealth-enabled care coordination with larger regional systems are doing two things simultaneously: improving access for their communities and creating the financial structures that make their own facilities more viable. The organizations that build these partnerships deliberately and on their own terms will be far better positioned than those that enter them under financial duress.
Build employer partnerships as a revenue and access strategy. Rural hospitals sit in the center of local economies dominated by agricultural operations, manufacturers, processing facilities, and service industries — many of which have workforces with significant healthcare needs and no local clinical solution. Employer-based clinic partnerships, occupational health programs, and transparent self-pay pricing structures for common services are revenue diversification strategies that rural hospitals are uniquely positioned to develop. These are not urban market concepts — they are access and revenue opportunities specific to rural market dynamics, and they are fundable under RHTP's provider payment and care access provisions.
The Vantage Perspective
RHTP is a resource. The operational architecture is what makes it last.
At Vantage Clinical Partners, we work alongside rural health systems and critical access hospitals to translate transformation funding into durable operational improvement. The organizations that will generate the most value from the RHTP are the ones that pair their investment strategy with the operational infrastructure to make it work — not just in year one, but across the five-year window and beyond.
Our Discovery & Planning work in rural settings surfaces the same opportunities repeatedly: workforce structures with retention levers that have not been fully activated, service lines with real community demand that lack the operational design to deliver them sustainably, and employer relationships in the local market that have never been formalized into clinical partnerships. These are not theoretical opportunities. They are investable ones — and the RHTP provides the funding context to act on them now.
That is the Implementation and Sustainment work we do alongside rural health leaders: turning a well-designed transformation plan into a care model that performs, retains talent, serves the community, and operates sustainably when the funding window closes.
The $50 billion Rural Health Transformation Program is a generational investment in communities that have long operated with fewer resources, thinner margins, and greater community dependence than any other sector of American healthcare. The rural health leaders who approach it as a strategic opportunity — who move early, invest deliberately, and build the operational structures that extend the impact beyond the funding window — will define what rural healthcare looks like for the next decade.
Beth Papetti, MBA FHM
Principal & Chief Operating Officer
References
American Hospital Association. (2026, March 2). Medicaid coverage supports rural patients, hospitals, and communities.https://www.aha.org/fact-sheets/2026-03-02-medicaid-coverage-supports-rural-patients-hospitals-and-communities
Center for Children and Families, Georgetown University. (2026, May 1). Rural hospitals and communities feeling impact of H.R. 1 Medicaid cuts, rural health fund falls short.https://ccf.georgetown.edu/2026/05/01/rural-hospitals-and-communities-feeling-impact-of-h-r-1-medicaid-cuts-rural-health-fund-falls-short/
Center for Healthcare Quality and Payment Reform. (2026, January). Rural hospitals at risk of closing.https://chqpr.org/downloads/Rural_Hospitals_at_Risk_of_Closing.pdf
Center for Healthcare Quality and Payment Reform. (2026). Stopping the loss of rural maternity care.https://ruralhospitals.chqpr.org/Maternity_Care.html
Chartis. (2026, February 10). 2026 rural health state of the state.https://www.chartis.com/insights/2026-rural-health-state-state
Centers for Medicare & Medicaid Services. (2026, March 3). CMS announces $50 billion in awards to strengthen rural health in all 50 states [Press release]. https://www.cms.gov/newsroom/press-releases/cms-announces-50-billion-awards-strengthen-rural-health-all-50-states
Centers for Medicare & Medicaid Services. (2026). Rural Health Transformation (RHT) Program overview.https://www.cms.gov/priorities/rural-health-transformation-rht-program/overview
KFF. (2025, September 25). A closer look at the $50 billion rural health fund in the new reconciliation law.https://www.kff.org/medicaid/a-closer-look-at-the-50-billion-rural-health-fund-in-the-new-reconciliation-law/
National Rural Health Association. (2026, April 24). NRHA statement for the record: FY 2027 HHS budget.https://www.ruralhealth.us/nationalruralhealth/media/documents/advocacy/2026/nrha-sfc-statement-for-the-record-fy-2027-hhs-budget.pdf
NSI Nursing Solutions, Inc. (2026). 2026 NSI national health care retention & RN staffing report.https://www.nsinursingsolutions.com/documents/library/nsi_national_health_care_retention_report.pdf