
Dynamic Tension as a Performance Engine for C-suites & Hospital Medicine Teams
Hospital C-suites & Hospital Medicine programs want the same things. High-quality care for every patient. An inpatient operation that moves efficiently. A team that is fully engaged, clinically excellent, and right-sized. Costs that reflect the value being generated. These are not competing priorities. They are a shared destination, and the dynamic tension between a hospital medicine group and the C-suite exists not because they disagree on where they are going, but because each sees a different set of obstacles standing between here and there.
That distinction matters enormously. When the tension is framed as a “values conflict” — clinical mission versus financial performance — it produces defensiveness, entrenchment, and the same unresolved conversation. When it is framed as a shared diagnostic challenge — two parties who see different parts of the same problem, whose combined visibility is greater than either has alone — it becomes something productive. It becomes the engine of a better-running inpatient medicine chassis.
The organizations that get this right do not eliminate the tension. They build the operational structure that channels it — turning the honest frustrations of both parties into a shared improvement agenda and turning the gap between what each side sees into a shared accountability framework. That is the work. And it starts with naming what each party is actually experiencing.
Ask hospitalists and HM advanced practitioners what frustrates them most, and the answer is barriers to patient progression. This is the core frustration: that when the hospitalist or advanced practitioner exerts clinical leadership — communicate discharge disposition 48-24 hours in advance, identifies the discharge criteria, names the barriers explicitly, writes the discharge orders — there is often not a designated individual to accomplish the work in a specified time period which leaves the operational response appearing often slow or fragmented. Barriers are discussed in huddles and noted in the chart. What is rarer is having someone whose explicit job is to take those barriers off the physician's list and resolve them in real time, so the patient moves and the bed opens and the next patient can come in. Hospitalists know that it is their job to help identify barriers in advance of the day of discharge; they want a partner who removes them once they are identified.
The C-suite's experience of the same operational reality often looks different. They see LOS data that is not moving as expected. They see readmission rates that are stubborn. They see ED boarding times that reflect a hospital that cannot turn over beds fast enough. They see quality metrics that should be improving and are not. And they often experience the hospital medicine program not as the solution to those metrics but as a contributor to the problem — because the program's connection to those outcomes has not been made explicit and because the c-suite does not have full visibility into the clinical and operational barriers the program is navigating every day. What the C-suite is asking for is demonstrated movement. Evidence that the hospital medicine program is driving the metrics that matter. A sense that every member of the group, not just the medical director, is operating with ownership and engagement. A program that feels like a partner in solving the organization's inpatient challenges rather than a team that surfaces problems without being part of the solution. It is relational and operational.
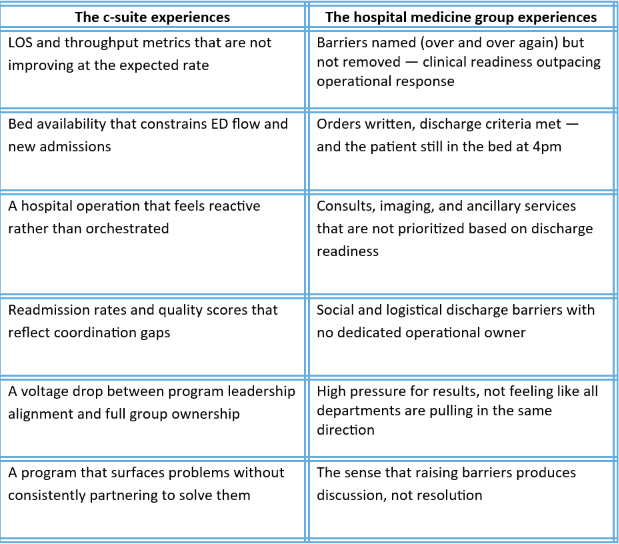
Both experiences are legitimate. Both are also incomplete — because neither party has full visibility into what the other is navigating. The C-suite does not always see the operational friction that the hospitalist is absorbing every day. The hospital medicine group does not always see how its collective activities read from the organizational leadership's vantage point. The shared frustration of the hospital medicine group and the c-suite converge on a set of operational gaps that neither party can close on their own — and that most hospitals have not systematically addressed.
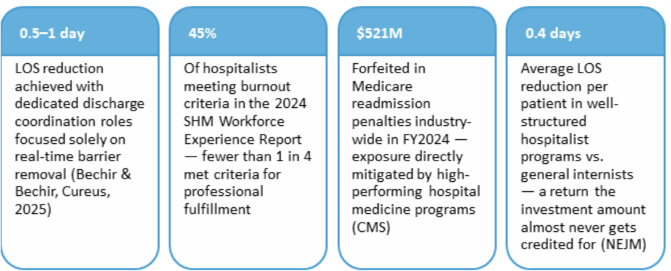
The barrier removal gap research published in The Hospitalist documents the impact of dedicated expediting teams — an expediting nurse, physician, and discharge nurse whose explicit function is to identify and remove discharge barriers in real time, beginning each morning with a secure message to rounding hospitalists asking for every known barrier to discharge, then escalating through defined pathways to the relevant departments. The result is not just a faster discharge. It is a fundamentally different relationship between the hospitalist and the organization: one in which the physician's clinical leadership is met with operational partnership rather than absorbed into the general noise of a busy floor.
A complementary body of evidence, synthesized in a 2025 Cureus review of 20 peer-reviewed studies, documents that dedicated discharge coordinators — nurses, nurse practitioners, or case managers focused solely on same-day discharge barrier resolution — reduce LOS by 0.5 to 1 day. The discharge coordinator functions as what the authors call the operational "traffic controller" of inpatient flow: not directing clinical care, but ensuring that the non-clinical tasks — imaging, consults, transportation, post-acute placement, documentation — align with the physician's discharge timeline rather than drifting on their own schedule.
Most hospitals have case managers. Far fewer have a role explicitly accountable for real-time barrier removal, empowered to escalate on behalf of the physician's order timeline and measured on same-day discharge completion. That gap is where patient days are being lost — not to clinical complexity, but to opportunity for better coordination.
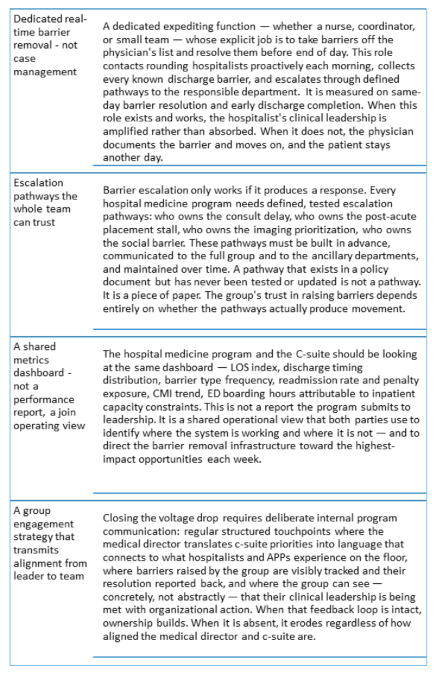
The structure that makes this work is not necessarily a scoreboard or an investment renegotiation that ties more dollars to metric performance. It is an operational architecture that closes the gaps both parties are experiencing simultaneously — giving the hospital medicine group the real-time operational partnership it needs to exert clinical leadership effectively, and giving the c-suite the shared metrics, visible engagement, and program accountability it needs to see the return on that partnership.
The Vantage Perspective
Same goals. Different views of what is in the way. That is the whole problem — and the whole opportunity.
At Vantage Clinical Partners, we engage hospital medicine programs from the premise that the dynamic tension between the program and the c-suite is productive when it is channeled — and damaging when it is left to repeat itself. Our Discovery & Planning work begins with both parties: what does the hospital medicine group experience as the primary barriers to doing their best work, and what does the C-suite experience as the primary gaps in program performance and partnership? The answer to those two questions, held together, is the operational agenda.
What we consistently find is that the hospital medicine group wants to exert clinical leadership and be met with operational response. The C-suite wants to see ownership and movement in the metrics that matter. These are not in conflict — but the infrastructure to connect them almost never exists at the level of specificity and accountability that makes it actually work. The barrier removal function is vague. The escalation pathways have not been tested. The shared dashboard is a report rather than a joint operating view.
Our Implementation work builds that infrastructure: the expediting and coordination roles, the escalation pathways, the shared metrics framework, and the group engagement structures that transmit alignment from the medical director to every hospitalist and APP on every shift. That is how dynamic tension becomes improvement. That is how both parties get what they are actually needing from one another.
What remains is to build the structure that uses that visibility well — that removes barriers in real time, that transmits ownership from leader to team, that makes the program's value legible and continuous, and that gives both parties the experience of genuine partnership rather than parallel frustration.
That structure is buildable. The gap between where most hospital medicine programs operate and where they could operate — when the tension between them and the C-suite is channeled rather than repeated — is one of the most significant and most underutilized performance opportunities in inpatient operations today.
Beth Papetti, MBA FHM
Principal & Chief Operating Officer
References
Bechir, G., & Bechir, A. (2025). Reducing delays, improving flow: The importance of a dedicated discharge coordinator in hospital discharge planning. Cureus, 17(6), e85879. https://doi.org/10.7759/cureus.85879
Centers for Medicare & Medicaid Services. (2024). Hospital Readmissions Reduction Program (HRRP). https://www.cms.gov/medicare/quality/initiatives/hospital-quality-initiatives/readmissions-reduction-program
Lindenauer, P. K., Rothberg, M. B., Pekow, P. S., Kenwood, C., Benjamin, E. M., & Auerbach, A. D. (2007). Outcomes of care by hospitalists, general internists, and family physicians. New England Journal of Medicine, 357(25), 2589–2600. https://doi.org/10.1056/NEJMsa0706947
Society of Hospital Medicine. (2024). 2024 Hospital medicine workforce experience report. https://www.hospitalmedicine.org/globalassets/practice-management/practice-management-pdf/pm-24-0018-workforce-experience-report.pdf
Tella, S. H. (2025, May 1). Can expediting patient discharge past clinical and non-clinical barriers improve overall hospital throughput? The Hospitalist. https://www.the-hospitalist.org/hospitalist/article/38647/key-operational-question